Dermatology Practice Reactivates 1,800 Dormant Patients in 90 Days

A dermatology practice was planning a fourth office, and they needed $1.4 M in incremental revenue. They wanted to improve their recall campaign for this revenue, as it was the only quick possible source of revenue.
Business Challenges
Dr. Carolyn Reese had been planning Solano Dermatology's fourth office for two years. The site was leased. The construction timeline was set for Q3. The financial pro forma needed $1.4M in incremental annual revenue to support the expansion — and the practice's organic patient-acquisition channel couldn't credibly generate it within the timeline. Paid acquisition was running $182 per new patient and had been compressing for six quarters as competitor practices in the Denver metro raised digital spend.
Solano's 12,400 active-record patients, 8,400 had not been seen for an annual skin check in 18+ months. The practice's clinical demand for skin-check appointments was outstripping capacity, and yet 68% of the existing patient base was sitting dormant. The math on recall as a growth lever was extraordinary: at typical dermatology reactivation conversion rates, the dormant cohort could generate $2M+ in visit revenue alone, plus a meaningful downstream Mohs and cosmetic mix.
The reason the practice hadn't been done was operational. The EMR's recall report was static — a list of names, no contact tracking, no campaign tooling. Front desk staff didn't have the bandwidth to make recall calls. Solano had attempted recall outreach twice in five years; both attempts had died within a month of being launched. Without a system that did the recall outreach automatically and tracked the response, the recall lever couldn't be made operational.
- Fourth office expansion required $1.4M incremental revenue with a Q3 deadline; paid acquisition couldn't credibly generate it within the timeline.
- 8,400 patients had not had a skin check in 18+ months despite practice demand outstripping capacity; the dormant cohort represented 68% of the active patient base.
- Paid-acquisition CAC sat at $182 and had been compressing; competitor digital spend in the Denver metro was eroding paid-channel efficiency.
- EMR's recall report was static (name list only); two prior internal recall attempts had failed because no outreach automation existed.
- Front-desk staff had no bandwidth to make recall calls; cosmetic and Mohs revenue was concentrated in 22% of the patient base.
Solution
Tony ran the procurement. His evaluation was structured around one specific question: which platform could execute a 90-day reactivation campaign against the 8,400-patient dormant cohort with the front-desk team's existing capacity?
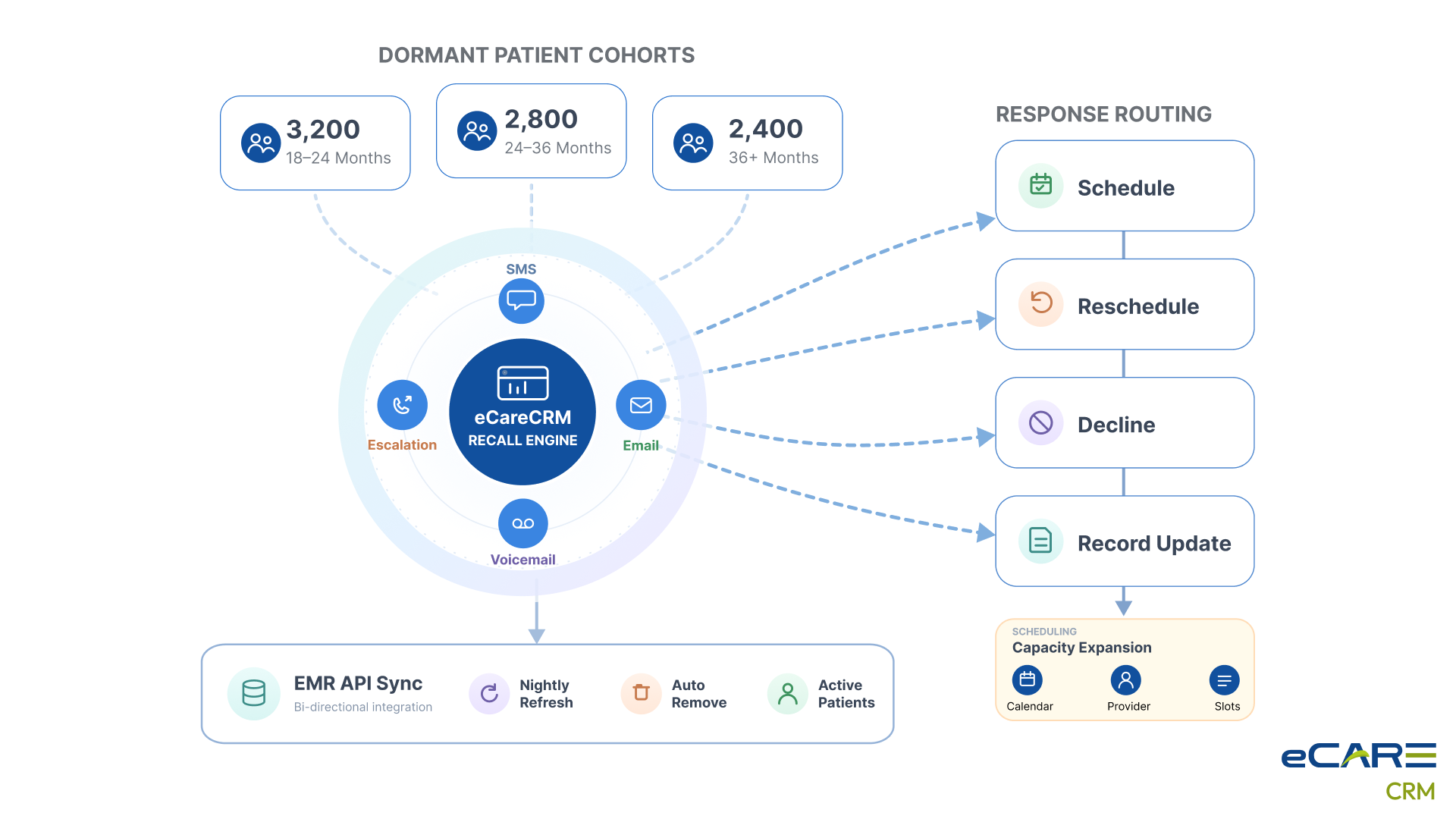
The selection moment came during the eCareCRM proof-of-value session. The eCareCRM team built a sample multi-touch sequence — SMS, email, voicemail-drop, and human-call escalation — against a sample slice of Solano's dormant cohort. They walked Tony through how the platform routed each patient's response to the appropriate downstream workflow (schedule, decline, reschedule-later, dispute-record). They showed him the per-touch reporting cockpit. Tony's response: "If this works at 15% conversion against 8,400 patients, it's the expansion." It became the expansion.
What also mattered was the integration model. eCareCRM connected to the practice's EMR through a structured API rather than a manual export workflow. The recall list is refreshed nightly. Patients who had been seen recently dropped off the recall list automatically. The system maintained its own state instead of relying on the front desk to keep it accurate.
Value Delivered
The 90-day campaign generated reactivation conversions at a rate that exceeded Tony's most optimistic projection. The patient cohort that hadn't been seen in 18+ months responded better to outreach than the cohort that had been seen in 12–18 months — counter to the operating assumption Tony had been carrying. The dormant patients had been waiting to be asked.
- 1,800 dormant patients reactivated in 90 days — a 21.4% response rate on the full 8,400-patient cohort.
- $1.4M in downstream visit, procedure, and cosmetic revenue from the reactivated cohort within the first six months.
- Per-reactivation cost of $42 against the $182 paid-acquisition CAC — the reactivation channel was 4.3x more efficient.
- Mohs case volume grew 28% in the quarter following the reactivation campaign as dormant patients with developing lesions came back.
- 3.3x ROI on the recall program in Q1 alone; the fourth office expansion proceeded on its original timeline.
Solution Provided
The deployment took 6 weeks — shorter than typical because the use case was specific. Tony ran it tightly. The eCareCRM team treated it as a tactical campaign deployment rather than a broad platform rollout.
Week 1: Cohort Segmentation
The 8,400-patient dormant cohort wasn't a single cohort. Tony and the eCareCRM team segmented it: patients last seen 18–24 months ago (3,200), 24–36 months (2,800), and 36+ months (2,400). Each segment got a slightly different campaign sequence — the most recently lapsed cohort got a soft skin-check reminder; the longest-lapsed got a more comprehensive welcome-back outreach.
Week 2: Campaign Sequence Build
The multi-touch sequence was built in week 2. SMS first (day 1), email follow-up (day 4), voicemail drop (day 8), and human-call escalation (day 12 — only to patients who hadn't responded to the prior three touches). The human-call list was sized to match the front-desk team's available capacity (approximately 40 calls per day).
Week 3: Pilot Against Segment 1
The 18–24-month cohort got the campaign first as a controlled pilot. The response was immediate — 287 bookings in the first week. The platform routed the bookings to the EMR scheduling layer automatically. The front desk handled the human-call escalations against the 14% non-responders.
Weeks 4–5: Segments 2 and 3
The two longer-lapsed cohorts came up next. The campaign sequences were adjusted based on Segment 1 learnings — Segment 3 (36+ month lapsers) received a longer email with a personalized note from Dr. Reese explaining why a skin check after a long gap mattered. The response rate held at 19–22% across all three segments.
Week 6: Scheduling Capacity Scale-Up
By week 6, scheduling was the constraint. The practice's existing schedule couldn't absorb the booking pace. Tony added Saturday morning slots for skin checks. Dr. Reese's two PAs picked up additional dermatoscopy capacity. The campaign continued generating bookings; the practice scaled to meet them.
Business Value
Solano's fourth office opened in October 2025 — on its original timeline, funded by the recall reactivation. Dr. Reese presented the engagement at a state dermatology society meeting later that year. The presentation was titled "The patients we already had."
What the practice learned about its own patient base
The operating assumption — that dormant patients were unreachable — was wrong. The dormant patients responded to outreach at higher rates than the recently-seen cohort responded to standard appointment reminders. The barrier hadn't been patient willingness; it had been the practice's inability to reach them systematically.
The financial picture
The $1.4M reactivation revenue funded the fourth office. The platform's recurring use has generated approximately $2.8M annually in retention and reactivation revenue against a $96K annual platform cost. The economics of the recall channel have made paid digital acquisition a secondary growth lever rather than a primary one.
What changed about the practice's growth thesis
Solano's expansion plan now centers on existing-patient revenue optimization before new-patient acquisition. The fifth office — already in planning — is being justified primarily by the per-patient revenue lift the practice can extract from its existing panel through structured engagement, not by net-new patient growth assumptions.
The line Tony uses internally
"We had been valuing patients on the date we last saw them. The dormant patients were the highest-yield reactivation cohort we could have built a campaign against. We had been ignoring our most valuable asset for years."

